How Red Light Therapy Can Accelerate Recovery After Traumatic Brain Injury
We aren’t making any claims in this article; we are simply sharing research.
This article examines whether red light therapy can support brain recovery and improve outcomes following traumatic brain injury.
Let’s take a closer look at red light therapy for concussion, known clinically as traumatic brain injury (TBI). This article reviews the available research and highlights how light therapy may meaningfully support the brain’s recovery process.
Rethinking How the Brain Recovers After Traumatic Brain Injury
To set the stage, let’s start with a few key facts about concussion and traumatic brain injury.
Statistics
Each year, just under 1% of the global population experiences a traumatic brain injury (TBI), amounting to roughly 70 million people worldwide (1). In developed countries such as the United States, the annual incidence is slightly lower, at around 0.7% (2). Of these cases, approximately 10% result in a hospital visit.
A small but meaningful proportion of TBI's are fatal (3). In the U.S., falls account for nearly half of all traumatic brain injuries, which helps explain why risk increases with age (4).
That said, TBI's are not limited to older adults. Children and teenagers also face elevated risk (5), and athletes are particularly vulnerable, with estimates suggesting that up to 10% experience a TBI each year (6).
Traumatic brain injuries exist on a wide spectrum, ranging from mild injuries, commonly referred to as concussions, to severe TBI's with far greater risk. Fortunately, the majority of cases are mild. However, recovery is not always straightforward. When symptoms persist for more than three months, the condition is often classified as post-concussion syndrome (PCS)(7). If symptoms continue even longer, it may be referred to as persistent post-concussion syndrome (PPCS)(8).
The terminology may vary, but the key point remains the same: for some individuals, the effects of a traumatic brain injury can linger for months or even years, significantly affecting quality of life.
For some individuals, the challenges of a traumatic brain injury do not fully resolve. Beyond the risk of long-term disability, severe TBI's are also associated with a higher risk of death (8). That increased risk is not limited to the immediate aftermath of the injury, but can extend years into the future, with elevated mortality observed even up to adecade later when symptoms persist (9).
Importantly, this risk is not confined to older adults. Younger people are also vulnerable, particularly those involved in contact sports. Activities such as soccer, football, and martial arts significantly increase the likelihood of concussion and traumatic brain injury during childhood and adolescence (10;11).
With that context in mind, let’s take a closer look at what the latest research reveals about these conditions and their recovery pathways.
Recent Scientific Reviews on Concussion
To ground this discussion in the strongest available evidence, this section draws on scientific reviews from the past six years. These reviews synthesize and evaluate high-quality research across the field. One particularly recent review offers a detailed overview of the biological processes that unfold in the brain following a concussion (12):
"After a concussion, a series of complex, overlapping, and disruptive events occur within the brain, leading to symptoms and behavioral dysfunction. These events include ionic shifts, damaged neuronal architecture, higher concentrations of inflammatory chemicals, increased excitatory neurotransmitter release, and cerebral blood flow disruptions, leading to a neuronal crisis."
A concussion causes real, physical changes within the brain. The severity of the injury largely determines how long the healing process takes. Unlike a broken bone, the damage from a concussion is not usually visible on standard imaging, but it is very much present. These changes occur across multiple levels, including inflammation, disruptions in neurotransmitter signaling, altered blood flow, and injury to brain cells themselves.
While many concussions do resolve on their own over time, thanks to the brain’s natural repair mechanisms and the typically limited extent of damage, recovery is not always straightforward. In some cases, symptoms persist, prompting further investigation. As another group of researchers explains:
"[The concept of persistent symptoms after concussion] emphasizes the fact that most persistent symptoms have their basis in complex somatic, cognitive, psychiatric, and psychosocial factors related to risk and resilience. This framework leads to the important conclusion that concussion is a treatable injury from which nearly all patients can be expected to recover." (13).
This conclusion cuts both ways. On the positive side, concussions are far better understood today than they were in the past, and their progression over time is easier to track and assess. At the same time, the wide range of possible symptoms highlights just how complex these injuries can be.
Post-concussion symptoms vary widely and can be difficult to summarize. Individuals respond differently to concussions, and no two injuries are exactly alike (14; 15; 16; 17; 18). The specific symptoms often depend on which areas of the brain are affected. For example, an impact to the back of the head may produce different effects than one to the sides or the occipital region.
Broadly speaking, post-concussion symptoms tend to fall into four main categories:
- Cognitive symptoms – These include brain fog or slowed thinking, reduced concentration, memory difficulties, mental fatigue, and decreased cognitive endurance.
- Physical symptoms – Common examples are nausea (reflecting the close connection between the brain and gut), fatigue, balance and coordination issues, visual disturbances, dizziness, and headaches. Physical and athletic performance may also decline significantly.
- Emotional changes – Some individuals experience increased anxiety, depressive symptoms, mood instability, or noticeable changes in personality and emotional regulation.
- Sleep disturbances – These can range from excessive sleepiness to poor-quality or fragmented sleep, disruptions in the normal day–night (circadian) rhythm, or a persistent sense of exhaustion regardless of sleep duration.
One of the challenges in managing concussion is that many symptoms remain inherently subjective (19). Unlike conditions such as stroke, epilepsy, or Alzheimer’s disease, which often produce clear and measurable changes on imaging or diagnostic tests, there is no definitive gold standard for quantifying concussion severity. Conventional imaging techniques such as MRI and CT scans typically cannot detect a concussion. As a result, diagnosis and assessment often rely on self-reported symptoms, observed behavior, and factors such as the duration of unconsciousness.
This subjectivity also makes persistent post-concussion symptoms difficult to measure and track over time (19).
Despite these challenges, a wide range of treatment approaches for concussion are currently used or under investigation (20):
"The use of osteopathic manipulative medicine(OMM), pharmacotherapy, hyperbaric oxygen therapy(HBOT), aerobic exercise, balance, and/or vestibular therapy are many common treatment approaches for concussion and post-concussion sequelae."
Several emerging interventions show promise for concussion recovery. Creatine supplementation has gained attention as a potential support for brain energy metabolism (21). Gradual, appropriately guided physical activity is also increasingly recognized as beneficial rather than harmful in many cases (22). Cognitive rehabilitation and psychological support, including cognitive behavioral therapy, may further help individuals manage symptoms and improve functional recovery (23). Encouragingly, the range of evidence-based treatment options continues to expand.
Looking ahead, advanced imaging approaches that assess cerebral blood flow, glucose utilization in the brain, and levels of neuroinflammation may help provide more objective measures of concussion severity and recovery timelines (24).
Key Insights from Recent Traumatic Brain Injury Reviews
Next, it’s helpful to look at what recent review papers tell us about traumatic brain injury more broadly. Moderate and severe TBIs often share symptoms with concussions, but these symptoms tend to be more intense and are frequently accompanied by additional complications.
Key differences include:
- Detectable changes on brain imaging – Unlike concussions, moderate and severe TBIs often show visible alterations on MRI or CT scans.
- Greater cognitive impairment – This may involve difficulties with speech, planning, decision-making, or overall cognitive function.
- More pronounced physical decline – Mobility, coordination, and endurance can be more substantially affected.
- Higher rates of depression and anxiety – Emotional and psychological challenges are especially common.
- Speech impairments – In some cases, speech difficulties resemble those seen after a stroke.
- Autonomic nervous system disruption – This can lead to problems regulating bloodpressure, excessive sweating, or abnormal body temperature control.
Current research highlights cerebral blood flow and brain metabolism as central factors in understanding and treating moderate to severe traumatic brain injury (25). Severe TBIs are often associated with long-lasting health consequences, as summarized in the following review:
"1. Expectation of long-term outcome is an important factor in treatment decision-making for patients with severe traumatic brain injury (sTBI). 2. Favorable outcomes and full recovery after sTBI are possible, but mortality and unfavorable outcome rates are high. 3. sTBI survivors are likely to suffer from a wide range of long-term consequences, underscoring the need for long-term and multi-modality outcome assessment in future studies. 4.The quality of the scientific literature on long-term outcome after sTBI can and should be improved to advance treatment decision-making." (26).
Taken together, this highlights the need for improved treatment strategies. Early intervention is especially important, much like in stroke care, where timing can strongly influence outcomes (26; 27; 28). In addition to medical approaches, a range of non-pharmacological interventions is already being explored, offering additional avenues for support and recovery (29; 30).
With that foundation in place, the key takeaway is clear: concussions and moderate to severe traumatic brain injuries still require better, more targeted treatment options. Encouragingly, there has been a growing body of research in recent years examining the effects of red light therapy on brain health.
The next section explores what this emerging science reveals.
How Light Influences Brain Recovery: The Science Explained
For some neurological conditions, the current evidence is especially encouraging. Fibromyalgia and Parkinson’s disease are not able examples, where early human studies suggest meaningful, sometimes life-altering improvements. While additional research is still needed, these early intervention trials point to substantial therapeutic potential.
For other conditions, the picture is more mixed. In epilepsy, for example, human research is still lacking. In areas such as depression, sleep disturbances, migraines, and related neurological concerns, the evidence consistently shows benefit, though the effects tend to be supportive rather than transformative.
This naturally leads to the next question: what exactly does red light do in the brain? Can red light therapy meaningfully influence brain inflammation, cellular energy production, or recovery processes?
A large and growing body of research now explores what is known as photobiomodulation of the brain, more commonly referred to as red light therapy for brain health (31; 32; 33; 34; 35). While the precise mechanisms are still being actively studied, several core biological effects have been consistently identified (31; 32; 33; 34; 35):
- Activation of brain mitochondria – One of the most widely accepted mechanisms involves cytochrome c oxidase (CCO), a key enzyme in mitochondrial energy production. Mitochondria act as the brain’s energy generators, and supporting their function is central to cellular recovery and resilience.
- Reduction neuroinflammation – Red light therapy has been shown to lower pro-inflammatory biomarkers while increasing anti-inflammatory signaling in the brain. Chronic neuroinflammation plays a role in many neurological and neurodegenerative conditions, making this effect particularly relevant.
- Improved cerebral blood flow – Appropriate wavelengths of light can enhance blood flow in brain tissue. The leading explanation involves nitric oxide (NO) release, which helps dilate blood vessels and improve oxygen and nutrient delivery.
- Healthier regulation of reactive oxygen species (ROS) – ROS are natural byproducts of energy production. While excessive levels contribute to aging and cellular damage, balanced ROS signaling is essential for adaptation and repair. Red light therapy appears to help restore this balance.
- Support for neurogenesis and synaptic growth – Red light therapy can stimulate the production of brain-derived neurotrophic factor (BDNF) and other growth factors. These molecules support the formation of new neurons and strengthen connections between brain cells.
Taken together, these effects align closely with what is needed in concussion and traumatic brain injury recovery. After TBI, blood flow is often reduced, inflammation increases, and oxidative stress rises. At the same time, the brain benefits from mechanisms that promote repair, plasticity, and new neural connections. From that perspective, the biological rationale for red light therapy in brain injury is compelling.
Next, let’s examine what the scientific studies actually show.
Red Light Therapy for Concussion and Traumatic Brain Injury: Repairing the Brain from Within
Let’s begin by looking at the available human studies on red light therapy for concussion and traumatic brain injury.
The first study examined individuals with mild TBI, or concussion, using LED-based red light therapy applied transcranially, meaning the light was delivered through the skull (37). Participants completed 18 treatment sessions over six weeks, averaging three sessions per week. Improvements on neurocognitive testing were observed in two of the nine participants. A major limitation of this study, however, is that critical treatment parameters, such as wavelength, dose, and power output, were not reported, making the results difficult to interpret or replicate.
Next, another study focused on individuals with moderate traumatic brain injury (38). The outcomes of that study were as follows:
" Despite the small sample size, the change in [Resting State Functional Connectivity (RSFC)] from the acute to subacute phases of recovery was greater in [red light therapy]-treated than sham-treated participants, suggesting that acute-phase [red light therapy] may have an impact on resting-state neuronal circuits in the early recovery phase of moderate TBI."
- Resting-state functional connectivity (RSFC) refers to how different regions of the brain communicate with one another when a person is awake but not engaged in a specific task. In other words, the brain is at rest, yet still actively coordinating information. RSFC is commonly disrupted in neurological conditions and also declines with aging. In this study, improvements in RSFC were observed following treatment, although, once again, detailed information about the treatment parameters was limited, making interpretation challenging.
- Another study explored a very different approach, using 633 nm light delivered intravascularly, meaning directly into the bloodstream (39). This method typically requires clinical assistance, as it involves accessing a blood vessel to expose circulating blood to light. In this study, red light therapy reversed a condition known as crossed cerebellar diaschisis, where one region of the brain becomes functionally suppressed due to injury elsewhere. However, despite this neurological improvement, measurable gains in cognitive function were not observed.
- Next, a small study examined transcranial light therapy using devices emitting 810, 850, and 870 nm wavelengths (40). The treatment was applied through the skull and involved four former football players suspected of having chronic traumatic encephalopathy, a condition associated with repeated head injuries. Participants received light therapy three times per week for six weeks and showed overall improvement. Notably, these individuals were over 50 years of age, suggesting potential relevance even in long-standing or cumulative brain injury cases. An image from the study illustrates the treatment setup (41). As shown in the study, a range of early-generation devices was used. Despite the small sample size, participants demonstrated improvements in cognitive testing as well as overall indicators of brain health.
- Another study investigated the use of a 1,064 nm wavelength delivered at a relatively high power output of 250 mW/cm² in 11 individuals with traumatic brain injury (42). Each session delivered a dose of 40 J/cm², which falls in the moderate-to-high range. Treatments were administered once per week over an eight-week period. The researchers reported the following outcomes:
"All patients enrolled in this study protocol were able to tolerate the study procedures without any [Adverse Events]s or [Serious Adverse Events]. Nine out of eleven participants had clinically significant improvements in [the participant's rate of improvement] score (≥ +2)." (43)
Overall, the improvements observed in this study were substantial. It is also notable that relatively high light power outputs were well tolerated, with no significant safety concerns reported.
In addition, another intravascular study using 633 nm light demonstrated meaningful benefits (44). In this case, the light appeared to protect against carbon monoxide–related toxicity, a factor that can contribute to secondary injury processes after traumatic brain injury. This mechanism overlaps with other affected systems following TBI, including glutamate-related excitotoxic pathways.
Next, a larger human study examined transcranial application of 810 nm light in 68 patients with moderate traumatic brain injury (45). No adverse effects were reported, and several objective biomarkers of brain health improved. Researchers assessed measures such as radial diffusivity, meandiffusivity, and fractional anisotropy, which are sensitive indicators of microstructural brain changes and can detect injury-related alterations before they become visible on standard CT or MRI scans. Symptoms everity also improved, as measured by the Rivermead Post-Concussion Questionnaire (RPQ). Participants received three treatment sessions, each separated by at least a 12-hour rest interval. A comparison between the placebo and treatment groups on the RPQ highlights these improvements (46):
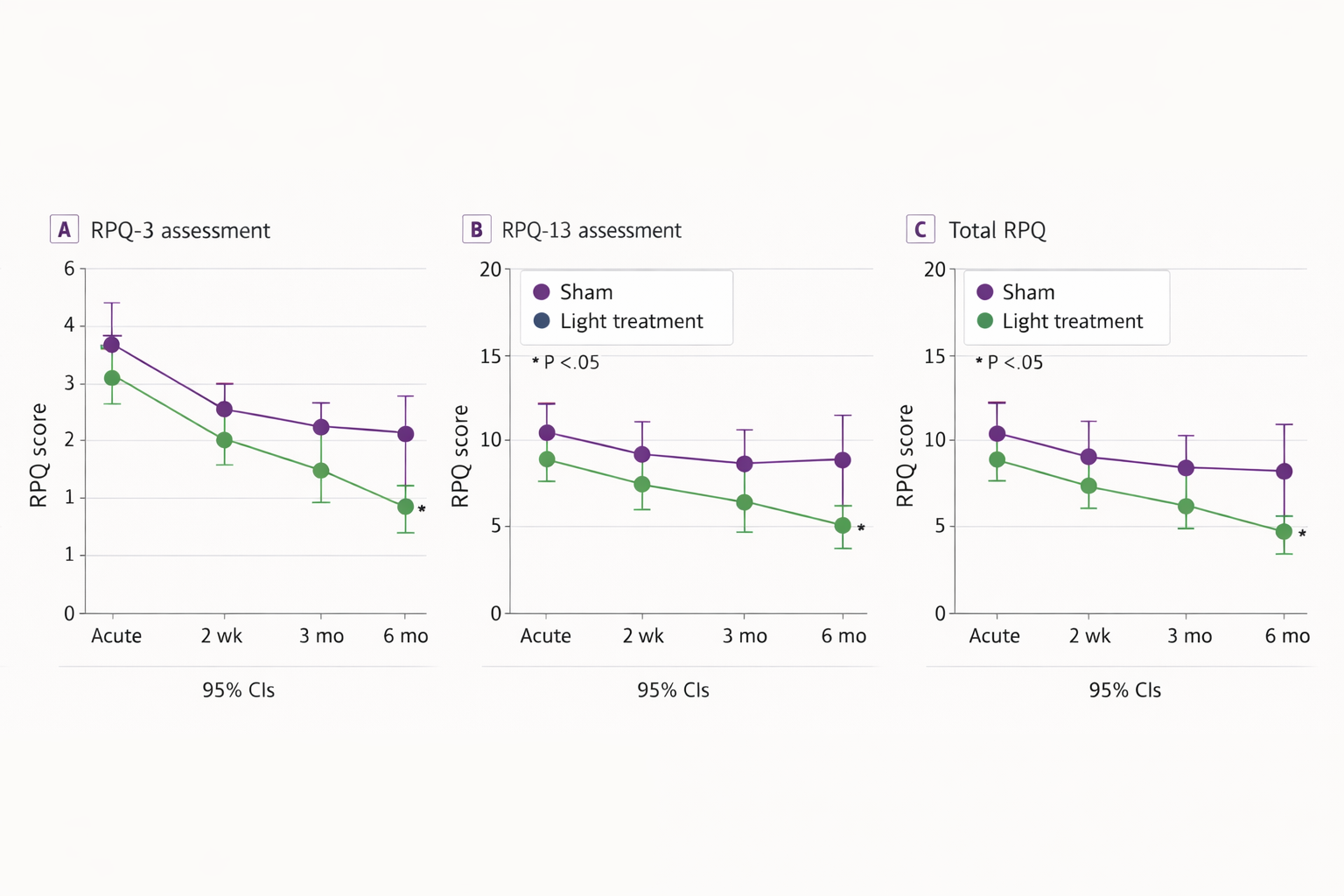
- These findings are particularly notable given the relatively small number of treatment sessions involved.
- Another study examined transcranial application of 630 nm light (47). In this case, cerebral blood flow increased following treatment, leading to improved oxygen delivery to brain tissue and subsequent gains in brain function. The study documented enhanced blood flow in both the left and right hemispheres of the brain, as illustrated in the accompanying imaging results (48).
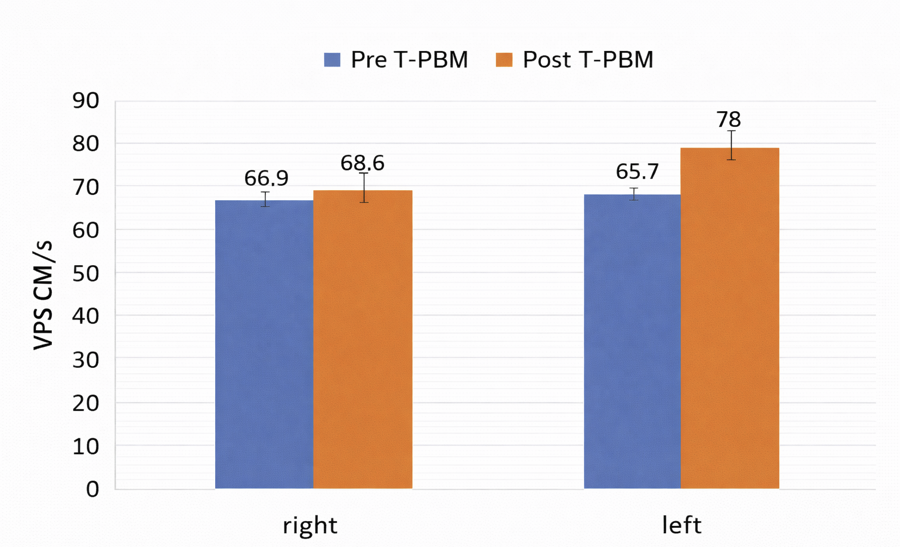
- One limitation of the study, however, is that long-term outcomes were not systematically tracked. Treatment was delivered three times per week over a three-week period, leaving questions about durability of the effects.
- Another study examined cerebral blood flow following transcranial light therapy using 630 nm and 810 nm wavelengths at relatively low power (6.4 mW/cm²) and a dose of 7.7 J/cm² (49). Despite the modest intensity, both cognitive function and cerebral blood flow improved, even though participants were treated years after their original traumatic brain injury. This finding suggests that red light therapy may still offer benefits well beyond the acute injury phase. In this study, participants received 18 treatments over three weeks.
- Finally, a case report explored the use of 810 nm and 980 nm light delivered over 20 sessions across two months (50). While this report involved only a single participant and included methodological limitations, such as likely misreported power output values, the clinical outcome described was nonetheless striking. The authors reported the following results:
"In this case report, a patient with moderate TBI documented in anatomical magnetic resonance imaging (MRI) and perfusion single-photon emission computed tomography (SPECT) received 20 NIR treatments in the course of 2 mo using a high-power NIR laser. Symptoms were monitored by clinical examination and a novel patient diary system specifically designed for this patient population. Clinical application of these levels of infrared energy for this patient with TBI yielded highly favorable outcomes with decreased depression, anxiety, headache, and insomnia, whereas cognition and quality of life improved." (50).
- In this context, SPECT imaging was used to assess cerebral blood flow (50). The results showed broad and meaningful improvements, making the findings particularly encouraging.
- Another study examined 11 individuals with chronic, mild traumatic brain injury who received light therapy using 633 nm and 870 nm wavelengths (51). Participants completed 18 treatment sessions over six weeks, with a dose of 13 J/cm² per session. Once again, the outcomes were highly positive, with the researchers noting the following:
"Participants reported improved sleep, and fewer post-traumatic stress disorder (PTSD) symptoms, if present. Participants and family reported better ability to perform social, interpersonal, and occupational functions. These open-protocol data suggest that placebo-controlled studies are warranted." (51).
- Another report describes a single-patient case study (52) in which transcranial light therapy was delivered using 23 LEDs at an 850 nm wavelength, with a total dose of 20 J/cm². Despite the small scale of the report, the outcomes were notable. Cerebral blood flow improved, and neurological symptoms showed meaningful recovery in a patient who had been in a vegetative state. It is important to note that this was a long-term intervention involving many treatment sessions, which may have contributed to the observed effects.
- Finally, another case study explored the use of 633 nm and 870 nm light for traumatic brain injury rehabilitation (53). Improvements were observed in cognitive function, and the treatment was administered at home. Beyond clinical benefits, the study also highlighted a reduction in overall treatment costs, suggesting potential advantages in accessibility and long-term care management.
What stands out from the studies above is a consistent pattern: the results are encouraging.
Across both red and near-infrared wavelengths, light therapy shows meaningful potential for traumatic brain injury, particularly in subacute and chronic cases. While there is limited data in the most severe, immediately life-threatening TBIs, longer-standing injuries appear to respond well, even to higher-powered applications. This suggests that the brain may remain responsive to photobiomodulation well beyond the initial injury window.
Something to note is that protocols in these studies vary widely, ranging from intravascular 633 nm applications to high-power 1,064 nm helmet systems and transcranial 810 nm devices. Despite this variability, the fact that positive outcomes emerge across such different approaches is itself a compelling signal. The science points in one direction: light therapy holds real promise in traumatic brain injury recovery.
Red Light Therapy for TBI: Insights From Scientific Reviews
Lastly, let’s look at several recent review papers on red light therapy for traumatic brain injury. As mentioned earlier, review studies synthesize and evaluate multiple high-quality investigations to provide a clearer, big-picture understanding of a topic.
For this section, I’ve focused specifically on the mos tup-to-date reviews available.
The first is a 2024 review, and here’s how the authors summarize the evidence:
"The outcomes in human clinical studies are then reviewed. The findings support [red light therapy] potential for treating TBI, notwithstanding variations in parameters such as wavelength, power density, dose, light source positioning, and pulse frequencies. Emerging data indicate that each of these parameters plays a role in the outcomes. Additionally, new research into [red light therapy]'s effects on the electrical properties and polymerization dynamics of neuronal microstructures, like microtubules and tubulins, provides insights for future parameter optimization. In summary, transcranial [red light therapy] represents a multifaceted therapeutic intervention for TBI with vast potential which may be fulfilled by optimizing the parameters."(54)
What’s notable is that the researchers are even more optimistic than many typical scientific assessments tend to be. In most cases, authors emphasize caution and call for larger, more standardized trials before drawing strong conclusions.
In this case, however, the confidence expressed in the findings stands out. The authors clearly view the existing data as compelling.
In addition, a particularly interesting 2022 review focused on animal research (55). While animal studies aren’t the focus of this article, they often provide important mechanistic insights, especially when human data is still emerging. This review specifically examined acute traumatic brain injury (55), and here’s how the researchers summarized those findings:
"For pre-clinical [a.k.a. animal] studies, [statistical] meta-analysis for [Neurological Severity Score] and lesion size were found to favor intervention versus control. Subgroup analysis based on [red light therapy] parameter variables for these outcomes was performed. Favorable parameters were identified as: wavelengths in the region of 665 nm and 810 nm; time to first administration of [red light therapy] ≤4 h; total number of daily treatments ≤3. No differences were identified between pulsed and continuous wave modes or energy delivery. Mechanistic substudies within included in vivo studies are presented and were found to support hypotheses of antiapoptotic, anti-inflammatory, and pro-proliferative effects, and a modulation of cellular metabolism. This systematic review provides substantial meta-analysis evidence of the benefits of [red light therapy] on functional and [cellular] outcomes of TBI in in vivo mammalian models."
It’s dense material, but the takeaway is encouraging. Even in acute traumatic brain injury, animal studies consistently show meaningful benefits when light therapy is applied within the first four hours after injury. These studies report reduced cell death (anti-apoptotic effects), lower inflammation, and enhanced cell repair and regeneration (pro-proliferative effects).
Taken together, these findings strongly support the potential role of light therapy in TBI recovery. Importantly, the conclusions from the most recent review papers closely align with the broader interpretation of the evidence so far.
With that foundation in place, it’s time to move on to another key piece of the puzzle.
Conclusion: A Promising Path Forward for Brain Injury Recovery
Whether delivered transcranially or intravenously, multiple forms of red light therapy have shown encouraging results for traumatic brain injury.
While more research is always wanted, the growing body of evidence is hard to ignore. More than a dozen human studies, supported by strong animal data, suggest that approaches to concussion and TBI care may evolve even more so over time.
The rationale is straightforward. Red light therapy is relatively low-cost, non-invasive, and has demonstrated measurable benefits across several studies. Although the effects may not be immediately transformative in every case, as seen with some other conditions, outcomes in TBI research are consistently favorable.
It is also reasonable to expect that longer-term treatment protocols, which have not yet been thoroughly studied, could yield even greater improvements. This makes the current findings particularly compelling.
Perhaps most reassuring is the safety profile: across published studies, outcomes are generally positive, and no serious adverse effects have been reported. Taken together, the evidence points toward a promising, low-risk adjunct in the evolving landscape of brain injury recovery.